- Home
- About Us
- Advanced Testing
- Nutrition & Self-Care
- Further Learning
- New Member Info
- Contact
CIMT testing is a specialized type of ultrasound that is done on the carotid arteries (in your neck) to assess the lining of these arteries. Regular carotid ultrasounds evaluate the blood flow in the neck (which would be affected by larger blockages), but a CIMT test can measure the actual degree of inflammation and plaque that exists in the lining of the artery. It can also differentiate between soft plaque (the dangerous kind that can rupture and lead to a sudden heart attack or stroke), and hard plaque (calcified plaque that is more stable but when large enough can obstruct blood flow and cause serious complications). CIMT measurements can be done every 6 – 12 months to follow the course of disease, helping to verify improvements from prescribed medical interventions, or document that the disease is worsening and the patient warrants more aggressive treatment.

Cardiovascular disease is the number one killer among both men and women in our nation, accounting for 33% of all deaths, and killing more people than all forms of cancer combined. 1 3 According to the American Heart Association, 50% of men and 64% of women who die suddenly of coronary vascular disease have NO previous symptoms. 4 12 In addition, as many as 50% of those who died from heart attacks or strokes had “normal” lipid profiles. 2
Atherosclerosis is a condition where fatty deposits collect and assimilate into the lining of the arteries, and can eventually form calcium deposits that block blood flow in the arteries. This can occur in patients without any obvious risk factors or symptoms. So we need to utilize better tools to identify and treat patients with hidden risk factors and CIMT is one of these tools.

The carotid arteries provide a “window” to the coronary arteries, and CIMT has been shown to be an independent predictor of future cardiovascular events, including heart attacks, strokes, and cardiac death. 6 Carotid IMT has the potential to catch more of these patients at risk, even in patients with normal EKGs, stress tests, echocardiograms and cholesterol panels.
Early detection is crucial so patients can be treated before they experience a heart attack or stroke. Prevention is the best treatment!
A CIMT test allows for earlier detection of atherosclerosis, helping the clinician more accurately risk stratify asymptomatic patients. Individual results from direct testing should always trump assessments that only consider risk factors, or only utilize a population-based risk calculator.
Studies have shown a 96% correlation between the disease found in the common carotid artery and the arterial disease found elsewhere in the body. There is a very high correlation between the thickness of the intima media and other risk factors, but CIMT has been shown to be more accurate in predicting disease than any other risk factor alone. In fact, CIMT measurement has been shown to be an independent risk factor for CV disease, even in the absence of any other identifiable risk factors. 6
A CIMT test helps identify inflammation in the lining of the arteries, in addition to measuring the severity of any existing plaque. This test also helps distinguish between the different types of plaque present, providing important information about stable and unstable plaque.
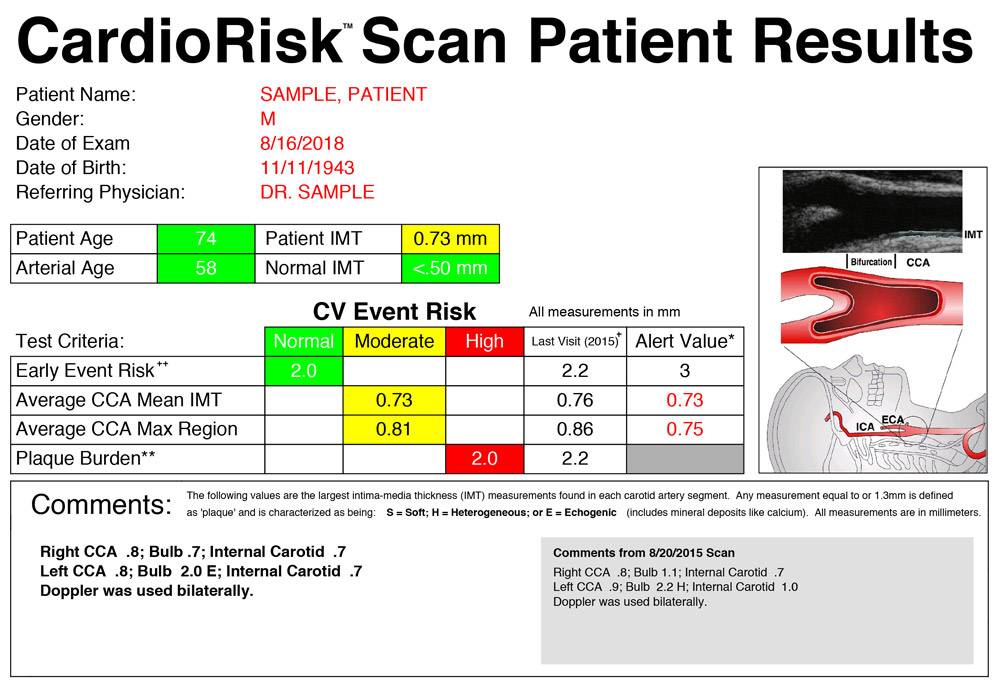
The CIMT report will include an estimate of the patient’s “vascular age.” It provides a measurement of how “old” the blood vessels are in comparison to other people the same age and gender. If the patient’s arteries are aging faster than expected, this may spur the medical provider to implement more aggressive lifestyle and medical interventions. Early detection can lead to early intervention.
Perhaps most important, is CIMT’s correlation and ability to predict coronary and cerebral events. CIMT was more accurate at predicting coronary artery disease than a CT angiogram of the heart! This may be due to the fact that plaque first begins to grow within the lining of the artery before it protrudes into the lumen (the interior of the artery) . . . so even an invasive coronary catheterization test with a cardiologist may not be able to identify soft growing plaque that is an active threat, because the plaque is not occluding the inside of the artery yet!
Healthy individuals can wait until age 45 to get a baseline, but any patient with risk factors (see list below) should consider getting one done sooner.
Family history of heart attack or stroke, or known genetic risk markers
Abnormal cholesterol (High LDL, low HDL, High triglycerides, High Lp(a), etc.)
Smoker
Diabetes, pre-diabetes, or metabolic syndrome
Overweight
High blood pressure
Sleep apnea
Erectile dysfunction
Pro-inflammatory state (i.e. elevated CRP)
Autoimmune disease (Lupus, Rheumatoid Arthritis, Psoriasis, inflammatory bowel disease, etc.)
Chronic unhealthy lifestyle (poor diet and lack of exercise)
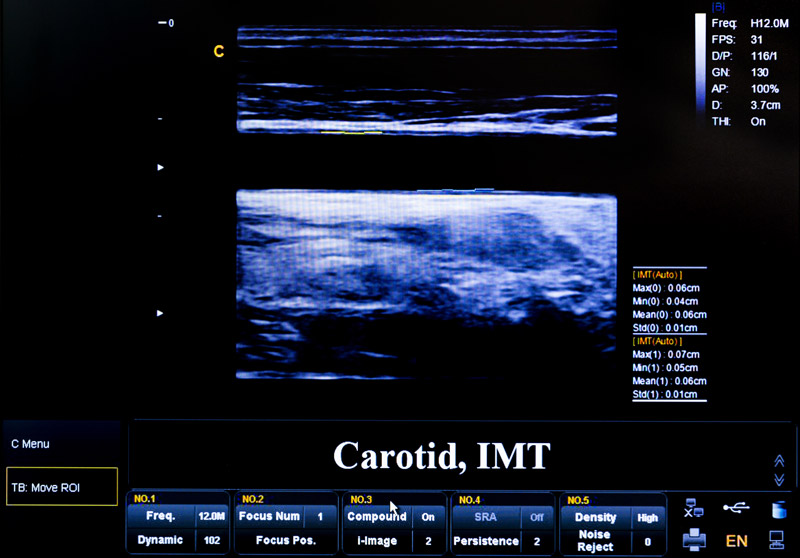
CIMT testing is a non-invasive ultrasound test that uses digital sophisticated edge detection software. The test is completely safe and painless and is done in-office. No disrobing is required, no needles are used, and there is no exposure to radiation. It typically takes only 10-15 minutes to perform.
After applying jelly to the skin over your neck, a small hand-held device is applied to capture images of the carotid arteries. The thickness of the inner layers of the artery is measured, in addition to any existing plaque (lesions > 1.3mm).

If a patient has an abnormal CIMT test, or identifiable risk factors, then the test should be repeated at least once a year. However, if lifestyle and medical interventions are made, then improvements can be seen as early as six months (so sometimes follow-up scans are done then). In healthy individuals who have normal CIMT results (and no risk factors or abnormal blood work), these patients can wait three years before getting another test done.
It is imperative clinicians use a quality Carotid IMT service in order to assure testing accuracy. When used properly, CIMT is more accurate in predicting CV disease than any other risk factor alone. However, the company must be able to reproduce comparable data over time, so we can accurately follow the course of arterial disease (and document whether it is improving or worsening). The quality of the equipment is important, but more so the training of the sonographer performing the test. A standardized scanning protocol must be used with CIMT testing, otherwise two different technicians could arrive at two different results. 8
At Whole Heart Family Medicine, we use Cardiorisk to do our scans. This company only uses experienced sonographers who are trained to employ a standardized scanning protocol. They also use ongoing quality control and quality assurance measures to guarantee reliability and reproducibility of results.

CIMT is a cost-effective diagnostic tool. The cost of a CIMT in our office is only $249 per scan, a small price to pay for the amount of information gathered. With appropriate diagnostic codes, insurance companies will cover the cost of a regular carotid ultrasound (assessing the blood flow through the carotid arteries), and this is sometimes needed in our higher risk patients . . . but this is different from a CIMT. Insurance companies do not currently cover the cost of a CIMT test, so in order to offer this test to our patients we simply charge the $249 fee up-front.
In patients with a normal CIMT, we may suggest they also get a FIMT (femoral intima-media thickness) test – this evaluates the large artery that supplies blood to your lower legs. Since plaque can collect in some arteries while leaving others untouched, additional arterial testing allows us to better assess a patient’s true risk. If this test is warranted, it can be added on for just an additional $149.
Other patients may benefit from an abdominal aortic ultrasound, particularly men over the age of 65 who have a history of smoking. This test can help accurately confirm or rule out the presence of an aneurysm and arterial plaque.
Finally, some patients may benefit from getting a coronary artery calcium score (CACS). This test is not covered by insurance either and costs around $140. Several studies have shown that a CACS is a better predictor of cardiovascular events than CIMT, particularly in patients with established atherosclerotic coronary artery disease. 7 “However, among patients with coronary micro-vascular dysfunction, CIMT seems to perform better than CAC score, so CIMT is a better earlier marker of disease.” 11
A coronary calcium score is a CT scan (specialized xray) of the arteries in your heart. Unlike a CIMT test, this test does expose the patient to a small amount of radiation. And unlike a CIMT, this test can only quantify calcified (hardened) plaque . . . which is identified in the later stages of arterial disease. Soft plaque (the more dangerous plaque that is vulnerable to suddenly rupturing and causing a heart attack or stroke) will not show up on a CACS.
In general, “patients with a CACS score of 0 have an excellent prognosis, with a 10-year event rate of about 1%.” 11 However, any CACS of 1 or above is considered a positive scan . . . evidence of plaque in the coronary arteries. These patients warrant more aggressive CV prevention (including daily statin and aspirin therapy).13 However, the cardiovascular risk increases as the score goes up. A score between 101-400 is considered moderate risk, and a score over 401 is considered high risk (and correlates with more than a 90% chance that plaque is blocking an artery in the heart). 9
Normally if a patient has plaque in their carotid arteries, then they will also have it in their coronary arteries (or vice versa), but this is not always the case. 7 So in patients with a normal CIMT scan, the CACS may help confirm whether a patient is at increased cardiovascular risk due to the presence of atherosclerosis. Read more HERE.
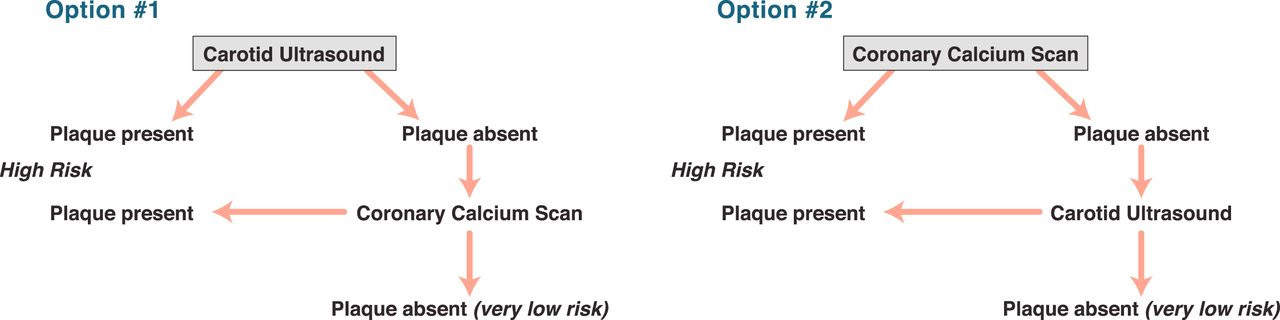
If the goal of screening is to simply identify subclinical atherosclerotic disease in 1 of 2 important vascular beds, then it would seem reasonable to start with carotid ultrasound first (because it is simple and safe with no radiation exposure and can be repeated at intervals to track changes in plaque with time and therapy), and if the study shows carotid plaque, then no additional screening may be needed. However, if the carotid study is negative, then it would seem prudent to proceed to imaging the coronary vasculature with a CT calcium scan as a preferred modality (see figure above). 7

The American College of Cardiology (ACC), American Heart Association (AHA) and Adult Treatment Panel of the National Cholesterol Education Program (ATP III) recognize CIMT as a reliable and safe means for assessing undetected vascular disease. Because the CIMT test can detect soft dangerous plaque in the coronary arteries before it is calcified, some feel CIMT is the best method to detect early disease. Unlike CACS, a CIMT test does not expose the patient to any radiation. In addition, the FDA and NIH accept CIMT (but not CACS) to follow the course of CV disease (help track progression over time). 10
CIMT testing has been used in research for over 20 years. It has been validated in many published studies in the most reputable journals, and has been used in large epidemiologic trials as well as large outcome studies as a surrogate end point for clinical events. However, it has only been available in the clinical settings since 2002.
In July of 2003, Dr. Pam Douglass, President of the American College of Cardiology recommended CIMT as an effective screening tool. This stems from the fact that 1) It is highly predictive for presence of coronary and cerebral disease. 2) It is highly predictive for the development of stroke, TIA and heart attack. 3) The relationship of carotid disease to disease of the coronaries is the same as one coronary to another. 4) Carotid IMT has the most data as a diagnostic tool for arteriosclerosis. (Transcript ACCEL interview – July 2003)
At its annual Prevention Conference V, the American Heart Association concluded that, “Carotid artery B-mode ultrasound imaging is a safe, noninvasive, and relatively inexpensive means of assessing subclinical atherosclerosis. The technique is a valid and reliable means of measuring IMT, an operational measure of atherosclerosis. The severity of carotid IMT is an independent predictor of transient cerebral ischemia, stroke, and coronary events such as MI . . . in asymptomatic persons > 45 years old, carefully performed carotid ultrasound examination with IMT measurement can add incremental information to traditional risk factor assessment.” 8
Do something today for a better tomorrow!
Make an appointment now for advanced testing. We are here to help.
REFERENCES
1 – Mozaffarian D, Benjamin EJ, Go AS et al. Circulation. 2015;131:e4-5,e282.
2 – Sachdeva et al. Am Heart J. 2009;157:111-117.e2
3 - Mozaffarian D, Benjamin EJ, Go AS et al. Circulation. 2015;131:e129.
4 – Kleindorfer D, Khoury J, Broderick JP, et al. Temporal trends in public awareness of stroke: warning signs, risk factors, and treatment. Stroke. 2009;40:2502-2506.
5 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5383538/
6 – https://www.ahajournals.org/doi/10.1161/01.CIR.101.1.e16
7 - http://imaging.onlinejacc.org/content/6/11/1168
8 - https://www.ahajournals.org/doi/10.1161/01.CIR.101.1.e16
9 – https://www.umms.org/ummc/health-services/diagnostic-radiology-nuclear-medicine/divisions-sections/computed-tomography-ct/cardiac-calcium-scoring
10 - https://www.cormedicalgroup.com/atherosclerosis-screening-with-carotid-imt/
11 - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4394551/
12 - https://www.uspharmacist.com/article/heart-disease-in-women-different-than-in-men
13 - https://www.acc.org/latest-in-cardiology/ten-points-to-remember/2018/11/09/14/28/2018-guideline-on-management-of-blood-cholesterol