November 12th, 2019
What is sleep apnea?
Sleep apnea is a potentially serious sleep disorder that causes breathing to repeatedly stop and start during sleep. The most common type of sleep apnea is obstructive sleep apnea (OSA) - it affects 34% of men and 17% of women in the United States. 1 Unfortunately, the grand majority of patients with sleep apnea remain undiagnosed and therefore at increased risk of many serious health problems. Uncontrolled OSA increases the risk of heart failure by 140%, the risk of stroke by 60%, and the risk of coronary heart disease by 30%. 2
How does sleep apnea occur?
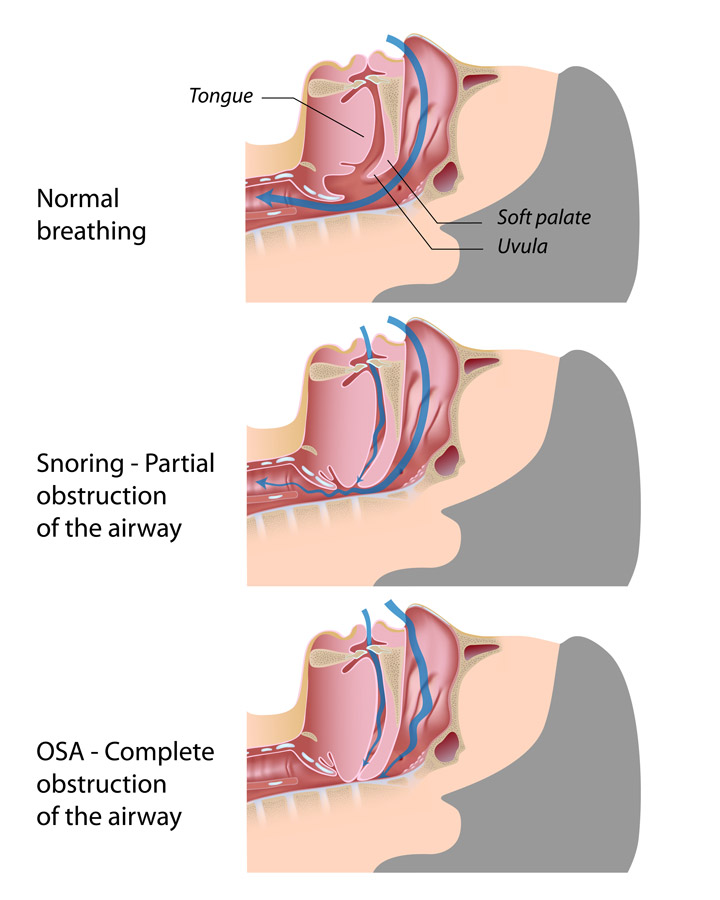
We all go through different stages of sleep at night, and our muscles relax during the deeper stages of sleep. In patients with OSA, this is problematic because the tongue and throat muscles relax to the point of obstructing the airway. This causes the patient to stop breathing, and as a result, oxygen levels drop. The body responds to low oxygen levels by triggering inflammation and releasing stress hormones like cortisol and epinephrine (also called adrenaline). Persistent elevations in adrenaline can lead to high blood pressure, so these repeated drops in oxygen levels end up putting stress on the heart and other organs. 3
The brain will not allow the individual suffocate when these obstructive events occur so it tells the body to breath. The individual then takes a deep breath and oxygen levels temporarily rise . . . but this sudden breath knocks the patient out of deep-stage sleep (though not necessarily awake, so the patient is often unaware this is happening). Now the patient is breathing, but they are no longer in the deeper stages of sleep (which the body needs), so the brain pushes the body back into deeper sleep. Then the airway obstructs . . . oxygen levels drop . . . so patient takes a deep breath . . . and this cycle repeats itself over and over all night.
Many important hormones and chemicals are produced during the deeper stages of sleep (vitamin d, testosterone, serotonin, dopamine, etc.), so these deeper stages of sleep (N3 and REM) are necessary for the patient to feel rested and function at their best.
Even if a patient sleeps eight hours, if their deep stage sleep is constantly disrupted throughout the night, then their body and brain are not getting restorative sleep, and they can wake feeling tired. Ideally adults need 7-8 hours of sleep a night, but the quantity of sleep is not nearly as important as the quality of sleep.
Does the severity of sleep apnea matter?
Apnea occurs when a person completely stops breathing for 10 seconds or longer. Hypopnea occurs when the airflow is not completely obstructed, but is significantly reduced, to the point that oxygen levels drop by at least 3%. The apnea/hypopnea index (AHI) quantifies the severity of OSA in each patient, explaining how many obstructive events occur each hour during sleep. Mild OSA is categorized by an AHI of 5-15, moderate is 15-30, and severe is over 30. However, do not be fooled because even “mild” sleep apnea can cause serious health problems. Just like a patient is not “mildly pregnant,” a patient with just “mild” sleep apnea still has a true sleep disorder that needs to be treated. Every obstructive event correlates with a drop in oxygen levels, which in turn puts extra stress on the heart and other organs. An AHI of 30 is certainly more detrimental than an AHI of 5, but both patients are in need of treatment.
What are the symptoms of sleep apnea?
Imagine if someone called you 10 - 20 times an hour all night long – think how this would make you feel the next day. Sleep apnea disrupts sleep in a similar fashion. The most common symptoms of sleep apnea are: dozing off when sitting still, feeling tired upon waking, and snoring loudly or gasping and choking while sleeping. People with sleep apnea can also experience morning headaches, feel irritable or depressed, have trouble concentrating, struggle to lose weight, have lower sexual drives, or find themselves waking up multiple times at night (even just to use the bathroom).
Because sleep affects nearly every system in our body, the patient’s overall health and quality of life can significantly improve by treating OSA . . . and the spouse’s quality of life can improve too (because treating OSA will stop the snoring). However, 25% of people with sleep apnea do not snore and are not overweight . . . so some patients with OSA do not fit the “typical” profile.
Can OSA cause serious risks or problems? Does it have to be treated?
Patients with OSA are at risk of many serious health complications. Accumulating evidence has linked OSA to multiple cardiovascular disorders including: hypertension, type 2 diabetes, coronary artery disease, stroke, heart failure and cardiac arrhythmias. OSA’s impact on CV disease appears to be due to cardio metabolic issues from hypoxia (low oxygen), sleep disturbance, and sympathetic nervous system surges (like adrenalin). These problems all culminate in elevated blood pressure and heart rate, endothelial dysfunction, systemic inflammation, and insulin resistance . . . all mechanisms involved in the pathogenesis of CV disease. 2 4
Unfortunately, sleep apnea is extremely under diagnosed today. About a third of the population has OSA, but most do not know it. If left untreated, OSA can put the patient at significant increased medical risks (at the minimum it doubles the patient’s risk of stroke or sudden cardiac death). So it is critical that patients get tested if they have any of the symptoms previously mentioned, or if their health care provider thinks they may be at risk.
How do I know if I have obstructive sleep apnea?
To determine if you have obstructive sleep apnea, you can go to an overnight sleep lab where they monitor your sleep cycles and oxygen levels while you sleep, or you can do a home sleep study test. (Read more HERE). The home tests are cheaper, and usually fairly accurate, but at times they can under diagnose the AHI, thus missing the milder cases of sleep apnea.
Sleep apnea can be positional, and is often the worst when sleeping on your back. So in order to accurately identify any obstructive events, it may be better for patients to sleep on their back during the sleep study.
Taking the STOP BANG questionnaire may help indicate whether a sleep study is needed.
How is obstructive sleep apnea treated?
The gold standard for treating OSA is with a CPAP (continuous positive airway pressure) machine. The newer machines are much smaller and quieter than they used to be, and even have the option for adding humidified air. In addition, there are many different masks to choose from (many smaller ones that only cover the nose). Most people adjust to wearing the mask within a few weeks, but if necessary, prescription medication can be given to help relax patient so they can better tolerate the CPAP at night. Ideally, people with OSA should wear their CPAP any time they are asleep (even if just napping); however, even just using it for 4-6 hours each night can greatly improve health and vitality.
At Whole Heart Family Medicine, we have found that patients initially resistant to using a CPAP often come back later touting improvements in physical and mental energy . . . so much so that they now refuse to go a night without using their CPAP. For some individuals, the difference can be life changing.

Will losing weight help treat my sleep apnea?
Weight loss can open up the airway and improve sleep apnea in many patients. For some, a 10% weight loss will decrease apneas by up to 50%. However, since weight loss does not help everyone, and OSA significantly increases a patient’s risk of cardiovascular disease, we recommend treating sleep apnea as soon as it is diagnosed. Then the patient can work on lifestyle changes . . . not the other way around. Using a CPAP will help restore deep stage sleep, which will help improve energy and restore metabolic balance, and this will make it easier to exercise and lose weight. If enough weight is lost, some individuals are able to discontinue CPAP treatment.
Are there other ways to treat OSA besides CPAP?
Some patients with sleep apnea will get improvement from using an oral device called a mandibular advancement device (MAD). These devices look very similar to sports mouth guards or orthodontic retainers. A MAD is a custom oral device that snaps over the top and bottom teeth and is connected by a hinge. The MAD works by easing the lower jaw forward, and in doing so, helps to stabilize the tongue and soft palate so the airway stays open during sleep.
Mandibular advancement devices are more effective in younger, thinner patients with just mild - moderate OSA. About a third of patients who use them get a 50% or more drop in apneas (usually the AHI drops by about 10). However, they do not work as well in patients with severe airway obstructions. 5
Avoid purchasing cheap over-the-counter oral devices to treat OSA because they are subpar. A qualified dentist who has had appropriate training in the field should provide a MAD. The dentist can then make fine tune adjustments for maximum benefit and comfort, and then redo the sleep study on the patient while they are wearing the MAD to assure it is working.
Read more about oral devices for OSA HERE.
What is positional sleep apnea?
Due to gravity, OSA is often worse when patients sleep on their back. However, some patients only have positional OSA, meaning they only have apneas when sleeping on their back. Patients can treat positional OSA by simply avoiding sleeping on their back. Sleeping on a foam wedge pillow may keep the patient on their side at night, but a better option might be a slumber bump, a Zzoma device, or a Nightshift sleep positioner. These devices are worn at bedtime to prevent the patient from rolling over on their back while they sleep.
REFERENCES
1 – Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, et al. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177:1006–1014.
2 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2546461/
3 - https://www.health.harvard.edu/heart-health/how-sleep-apnea-affects-the-heart
4 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5891150/
5 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5803051/
6 – https://www.alaskasleep.com/blog/dental-appliances-for-sleep-apnea


